
The Clinical Data Interchange Standards Consortium (CDISC) is a global not-for-profit organization that develops standards to support the acquisition, exchange, submission, and archive of data in clinical research. The mission of CDISC is to develop and support global, platform-independent data standards that enable information system interoperability to improve medical research and related areas of healthcare.
An important component of many clinical studies is the collection of Pharmacokinetic (PK) blood samples and the subsequent analysis of PK data. The CDISC standards most associated with the analysis and submission of PK data are the Study Data Tabulation Model (SDTM) and Analysis Data Model (ADaM). An example workflow incorporating SDTM and ADaM datasets in a typical CDISC compliant Pharmacokinetic (PK) analysis is illustrated in Figure 1.
Figure 1 Example SDTM and ADaM workflow associated with the submission of CDISC compliant PK datasets
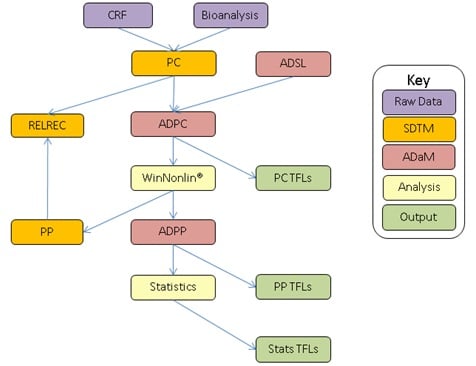
SDTM: Study Data Tabulation Model, ADaM: Analysis Data Model, CRF: Case Report Form data, Bioanalysis: Bioanalytical results dataset, WinNonlin: PK analysis software, TFLs: Tables, figures and listings.
Study Data Tabulation Model (SDTM)
As illustrated in Figure 1, there are currently two primary SDTM domains dedicated to the submission of PK data: the Pharmacokinetic Concentration (PC) domain and the Pharmacokinetic Parameter (PP) domain.
The PC domain is used for the submission of all concentration results (plasma and urine) and has a structure of one record per subject/dose/day/analyte/time point, hence concentration-time profiles are stored across multiple records. The PC domain ultimately forms the basis of the pharmacokinetic analysis used to derive multiple pharmacokinetic parameters for each individual Pharmacokinetic (PK) profile (such as Cmax, tmax, AUC, half-life, etc), which are subsequently submitted in the Pharmacokinetic Parameter (PP) domain. The PP domain has a structure of one record per PK parameter per concentration-time profile, and although the data presented are not considered to be observed data, the submission of PK Parameters fits well into the SDTM general observation class model. Indeed, most FDA reviewers prefer PK data to be submitted in the form of an SDTM dataset.
Analysis Data Model (ADaM)
Generating SDTM PP domains from SDTM PC domains is not quite as simple as it may seem. PK analyses typically require a number of variables which cannot be added to the SDTM PC domain (such as dose level, actual time relative to dosing, etc); therefore, it is not possible to simply feed SDTM PC into an appropriate software package (such as Phoenix WinNonlin) and generate derived PP data. In order to do this, an intermediate analysis dataset must be produced, and this is where we utilise ADaM.
ADaM standards essentially allow SDTM datasets to be transformed for analysis purposes, and in theory should always be ‘one procedure away’ from an output. The analysis of PK data generally involves the creation of two separate ADaM datasets: ADPC and ADPP. ADPC typically contains all relevant variables from SDTM PC, merged with ADSL (i.e. the primary subject level data such as demography and treatment information) and including additional variables required for the PK analysis (such as the actual time relative to the start of dosing for each PK profile). ADPC can then be fed directly into Phoenix WinNonlin (or alternative PK software packages) to derive the Pharmacokinetic (PK) parameters. These parameters are subsequently used to populate the SDTM PP domain, which in turn is merged with ADSL to create ADPP, the PK analysis dataset used in the statistical analysis of PK data (such as dose-proportionality and bioequivalence analyses).
Relating PC and PP Records
Once the SDTM and ADaM datasets have been created there is one more important consideration when submitting PK data in CDISC format, and that is the requirement to link all derived PP parameters back to the original PC observations. This link can be established in one of two ways: RELREC or ADaM.
The primary method to link PP and PC observations which is detailed in the SDTM IG (Study Data Tabulation Model Implementation Guide) is a RELREC table. The general concept of RELREC tables is that related records from each domain are presented in adjacent rows, with variables (such as IDVAR, IDVARVAL and RELID) used to link each observation together. However, the submission of records in RELREC can vary in complexity a great deal, and for this reason many sponsors prefer to link PC and PP records using the analysis metadata. As a result, the SDTM IG also states that sponsors may document those concentrations used to calculate each PK parameter via the analysis datasets (i.e. ADaM).
Conclusion
CDISC standards have been in place for a number of years to streamline the submission of clinical study data, and are expected to become mandatory for all regulatory submissions to the US Food and Drug Association (FDA) from 2016. CDISC compliant Pharmacokinetic (PK) workflows are therefore set to become increasingly important over the next few years, with benefits and efficiencies in store for sponsors familiar with the nuances of submitting PK data in a CDISC compliant format.
![The Creation of ADaM Datasets for Pharmacokinetic (PK) Analysis [Video]](https://www.quanticate.com/hs-fs/hubfs/Live%20Webinar%20Featured%20Image.jpg?width=390&name=Live%20Webinar%20Featured%20Image.jpg)


